
The effect of heart rate on amplitude change of vessel walls oscillations.
Well known that heart rate changes may occur under specific illnesses (i.e. cardiac arrhythmias) and with age.
Let’s introduce the following abbreviations:
m – Cardiac output
M – Vessel blood volume before arriving of a pressure wave
V1 – initial volume speed of vessel walls
V0 – volume speed of vessel blood intake
The picture below shows a general view of the process schematics:
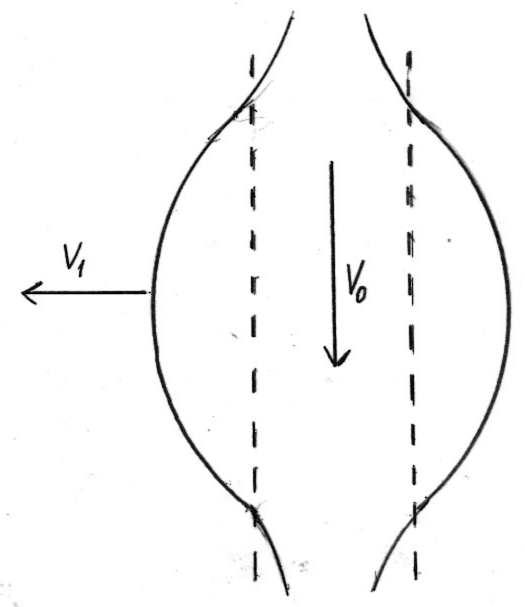
With passing of a wave of pulse pressure the vessel walls begin to stretch until the energy of motion transfers into the energy of deformation. Then the process will reverse itself and the shape of the vascular wall will be restored. Potential energy of the vessel walls will decrease and kinetic energy will increase. Let us assume that this transition is complete (absolute). Then:

k – force of resistance (a restoring force)
A2 – amplitude of vascular wall oscillation
From the energy conservation equation one can derive:

A magnitude of a restoring force which is applied to the walls is defined as:
where ω – rate of wall oscillation
or
x – wall deformation
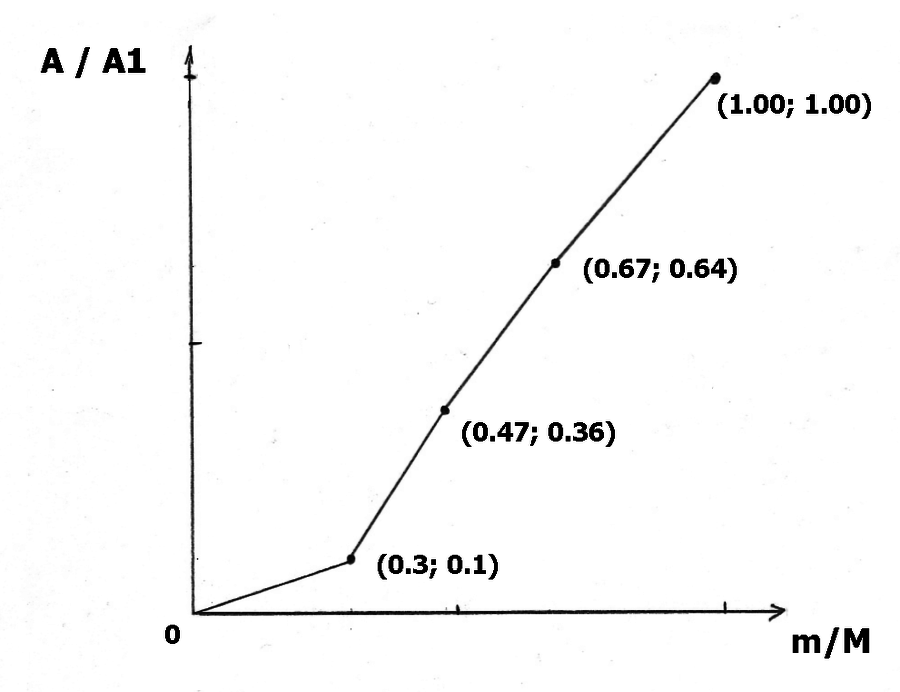
Therefore, this it is evident that under the small cardiac output the amplitude of the oscillation of a microvessel is decreasing. This in turn leads to a creation of a blockage of a mass (i.e. fluid) exchange between the extravascular fluid and the vessel walls. In other words, the decrease of the deformation value leads to the decrease of the intake of the extravascular fluid from the periphery, which in turn leads to an accumulation of the extravascular fluid.
The graph below shows the dependency of the amplitude of the oscillation of the vascular wall vs. a change of a cardiac output.
The dynamics of the cerebral regional brain extravascular extracellular fluid movement: implications
Age-related changes which lead to the weakening of the inotropy of the heart muscle may decrease the mass (fluid) transfer between the microvessel and the cerebral regional brain extravascular extracellular fluid due to the “deformation pump” effect. The deformation pump may play an important role in the functional deformity of the vascular wall due to the pulse wave movement. The mechanism of the deformation pump may open up new directions in our understanding of other pathologies with strong vascular component.
First, the cerebral regional brain extravascular extracellular fluid movement depends directly on the blood pressure pulsation in the vessels caused by the work of the heart. Second, the value of the velocity of the cerebral regional brain extravascular extracellular fluid movement depends on the blood pressure pulsations in the vessels: the higher the value of the amplitude of the pulsation the faster the velocity of the cerebral regional brain extravascular extracellular fluid movement. Third, the type of the pulsation of the blood pressure (accelerated or sharp) changes the velocity of the cerebral regional brain extravascular extracellular fluid input to the microvessels. Fourth, the larger the diameter of the oscillating vessel the faster the velocity of the cerebral regional brain extravascular extracellular fluid input. Finally, since heart rate affects the change in the amplitude of the oscillations of the vessel walls, it may directly affect the velocity of the cerebral regional brain extravascular extracellular fluid input to the microvessel walls.
The obvious implication of this mechanism is the primary involvement of cardiac function and atherosclerosis and therefore aging in the development of Alzheimer’s disease. Let us consider an example of Alzheimer’s disease and cardiac arrhythmia. On one hand, patients diagnosed with cardiac arrhythmias may benefit from early screening for Alzheimer’s disease (i.e. by testing the spinal fluid)[118]. On the other hand, if cardiac arrhythmias contribute to the worsening of existing Alzheimer’s disease and its prognosis, then a more aggressive treatment of arrhythmias should be considered. Finally, findings that suggest that cardiac function and Alzheimer’s disease are associated should raise the important question: What is it about this association that may further advance our understanding of Alzheimer’s disease?
In addition, pulse wave velocity itself can be reliably measured by an instrument called the pulse wave velocity/ankle brachial index. In a study of 96 patients with and without dementia, the values of velocity was found to be significantly higher among those with vascular dementia (p < 0.01)[119].
118] De Meyer G, Shapiro F, Vanderstichele H et al.
Diagnosis-independent Alzheimer disease biomarker signature in cognitively normal elderly people. Arch Neurol 2010; 67(8):949-56.
Notes: CORPORATE NAME: Alzheimer's Disease Neuroimaging Initiative
[119] Mizushima Y, Oobasawa H, Yoshida S et al. Pulse wave velocity in persons with vascular dementia. J Am Geriatr Soc 2003; 51(9):1329-30.
WAYS TO HELP:
We accept Bitcoin donations.
1PB3SeKNmA2DyMvBLUWXEYe4Pt3EvYFJHW
We also accept a donor-advised fund (DAF). You may wish to create such fund via Fidelity Charitable and select our non-profit.
Our EIN is 46-3208078
Did you know that life expectancy in the United States has declined? It happened again following last year's decline and for the first time in more than two decades!
Did you also know that the oldest man on Earth (who is now 123) lives in the mountains at an altitude of more than 12,000 feet?
But did you also know that previous large population-based studies found that residents of areas situated at 1500 m or above have longer life expectancy as compared to those who reside at sea level.
Read more about our research on aging and altitude. Answers that are yet to be found!
CMDAT stands for Complex Mechanisms of Disease, Aging and Trauma.
Did you know that CMDAT. Research Foundation is a 501(c)(3) not-for-profit organization, so your gift is tax deductible to the extent allowed by law?
We are also registered with the Benevity Causes Portal.