
Alzheimer's disease and cardiovascular pathology
The idea that ineffective left ventricular function and hemodynamic “instability” play an important role in the development of Alzheimer’s disease and vascular dementia has not been substantially developed. For instance, only a few population studies suggest that there is an association between atrial fibrillation and Alzheimer’s disease progression[51]. However, no serious consideration of the mechanism has been provided. More recently, Bunch et al.[52] observed that atrial fibrillation was associated with all dementia types and those aged 70 or younger were at highest risk. Nearly one third (10,161 or 27%) of the 37,025 study participants developed atrial fibrillation and 347 (0.94%) developed Alzheimer’s disease. More than a 2-fold increased incidence of Alzheimer’s disease was observed over the 5 year of follow up (0.7% vs. 1.5%, p-value < 0.0001).
In general, atrial fibrillation is considered to be the most common cardiac arrhythmia[52]. It is clinically important as patients diagnosed with atrial fibrillation are at higher risk for heart failure, and therefore compromised hemodynamics. Atrial fibrillation itself disrupts cerebral circulation leading to cognitive decline and dementia[53-55]. Finally, atrial fibrillation has been linked to all dementia types in previous studies. However, there is a lack of research evidence linking other common types of arrhythmia among the elderly. Namely, sinus bradycardia and sick sinus syndrome to the development of Alzheimer’s disease have not been examined. Sinus bradycardia may result in decreased cerebral blood flow and cerebral dysfunction[58-61]. Sick sinus syndrome is relatively rare condition which mostly affects the elderly. Similar to other types of arrhythmia, this syndrome can compromise normal hemodynamics possibly leading to disrupted cerebral blood flow.
In addition, both sick sinus syndrome and sinus bradycardia may produce episodes of hypotension and decreased cerebral blood flow velocity which, in turn, may result in increased blood viscosity and increased rouleaux formation (implications will be considered in the next chapter). On the other hand, hypotension induced by arrhythmias may lead to cerebral hypoperfusion[62].
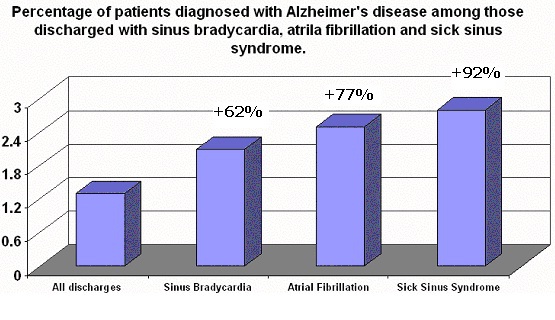
One way to estimate how many people are affected by this disease is to look at the large hospital discharge data which can be derived from the Healthcare Cost and Utilization Project Nationwide Inpatient Sample. The Nationwide Inpatient Sample contains a national all-payer data set with 7.45 million uniform hospital discharge abstracts for all inpatient stays in 2001. The detailed description of the data is available from http://www.hcup-us.ahrq.gov/db/nation/nis/Overview_of_NIS_2001_25Jul03.pdf. The important feature of this data is the availability of ICD-9-CM diagnosis codes. Other variables of interest include types and sources of admission, primary and secondary sources of payment and various patient-level characteristics. Using ICD-9-CM methodology, we calculated that there were 1,080 (0.015%) patients discharged with both sick sinus syndrome and Alzheimer’s disease and 2,760 (0.037%) patients discharged with both sinus bradycardia and Alzheimer’s disease in 2001.
A comparison chart presenting the proportions of patients diagnosed with both cardiac cause of hemorheologic “disturbance” (i.e. sinus bradycardia, atrial fibrillation and sick sinus syndrome) and Alzheimer’s disease is given below. The important finding using ICD-9-CM methodology was that the proportion of patients diagnosed with both sick sinus syndrome and Alzheimer’s disease was significantly higher (P < 0.001) compared to the proportion of those patients diagnosed with Alzheimer’s disease and any other discharge diagnoses, followed by the remaining proportions (i.e. atrial fibrillation and Alzheimer’s disease; sinus bradycardia and Alzheimer’s disease):
References
[51] Mielke MM, Rosenberg PB, Tschanz J et al. Vascular factors predict rate of progression in Alzheimer disease. Neurology 2007; 69(19):1850-8.
[52] Bunch TJ, Weiss JP, Crandall BG et al. Atrial fibrillation is independently associated with senile, vascular, and Alzheimer's dementia. Heart Rhythm 2010; 7(4):433-7.
[53] Knecht S, Oelschlager C, Duning T et al. Atrial fibrillation in stroke-free patients is associated with memory impairment and hippocampal atrophy. Eur Heart J 2008.
[54] Miyasaka Y, Barnes ME, Petersen RC et al. Risk of dementia in stroke-free patients diagnosed with atrial fibrillation: data from a community-based cohort. Eur Heart J 2007; 28(16):1962-7.
[55] Kilander L, Andren B, Nyman H et al. Atrial fibrillation is an independent determinant of low cognitive function: a cross-sectional study in elderly men. Stroke 1998; 29(9):1816-20.
[56] Ismailov RM, Ness RB, Redmond CK, Talbott EO, Weiss HB. Trauma associated with cardiac dysrhythmias: results from a large matched case-control study. J Trauma 2007; 62(5):1186-91.
[57] Jager TE, Weiss HB, Coben JH, Pepe PE. Traumatic brain injuries evaluated in U.S. emergency departments, 1992-1994. Acad Emerg Med 2000; 7(2):134-40.
[58] Fowler NO, Fenton JC, Conway GF. Syncope and cerebral dysfunction caused by bradycardia without atrioventricular block. Am Heart J 1970; 80(3):303-12.
[59] Walter PF, Reid SD Jr, Wenger NK. Transient cerebral ischemia due to arrhythmia. Ann Intern Med 1970; 72(4):471-4.
[60] Rasmussen K. Chronic sinoatrial heart block. Am Heart J 1971; 81(1):39-47.
[61] Ferrer MI. The sick sinus syndrome in atrial disease. JAMA 1968; 206(3):645-6.
WAYS TO HELP:
We accept Bitcoin donations.
1PB3SeKNmA2DyMvBLUWXEYe4Pt3EvYFJHW
We also accept a donor-advised fund (DAF). You may wish to create such fund via Fidelity Charitable and select our non-profit.
Our EIN is 46-3208078
Did you know that life expectancy in the United States has declined? It happened again following last year's decline and for the first time in more than two decades!
Did you also know that the oldest man on Earth (who is now 123) lives in the mountains at an altitude of more than 12,000 feet?
But did you also know that previous large population-based studies found that residents of areas situated at 1500 m or above have longer life expectancy as compared to those who reside at sea level.
Read more about our research on aging and altitude. Answers that are yet to be found!
CMDAT stands for Complex Mechanisms of Disease, Aging and Trauma.
Did you know that CMDAT. Research Foundation is a 501(c)(3) not-for-profit organization, so your gift is tax deductible to the extent allowed by law?
We are also registered with the Benevity Causes Portal.